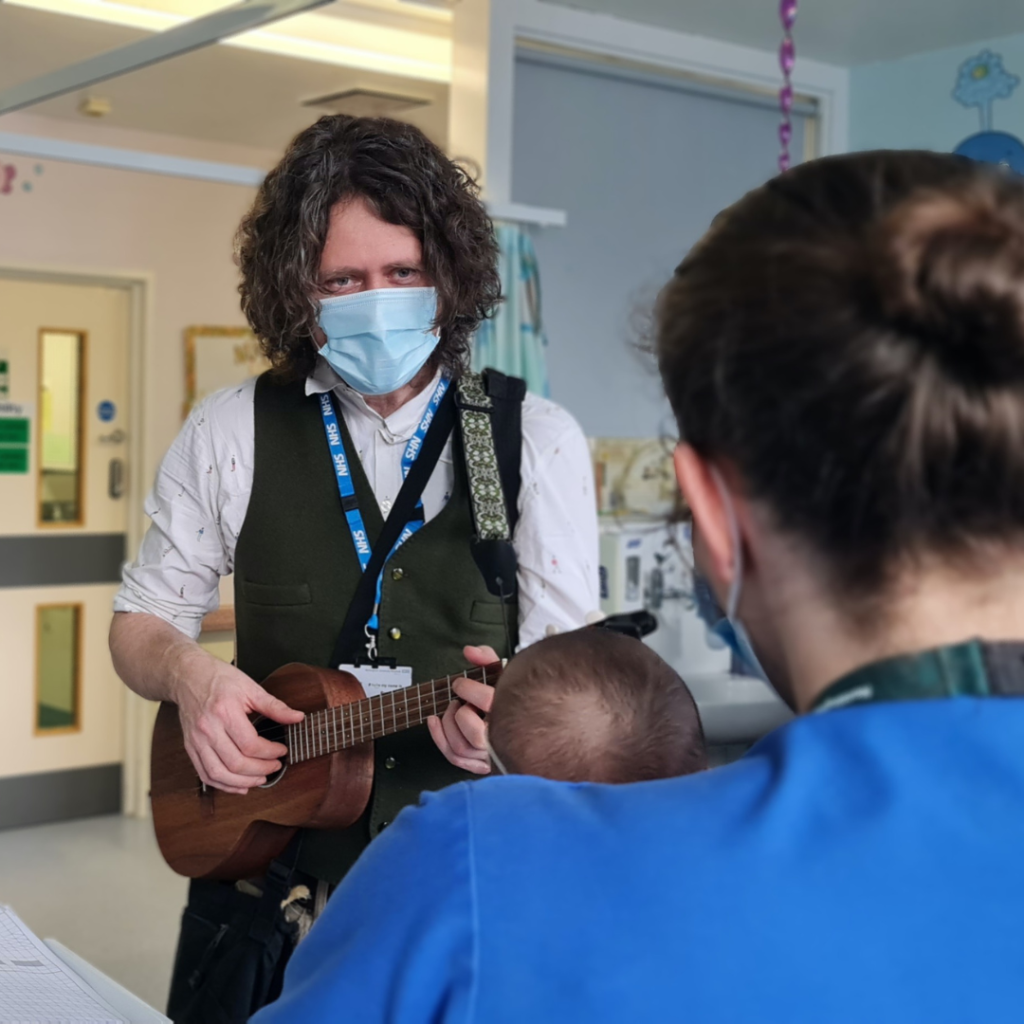
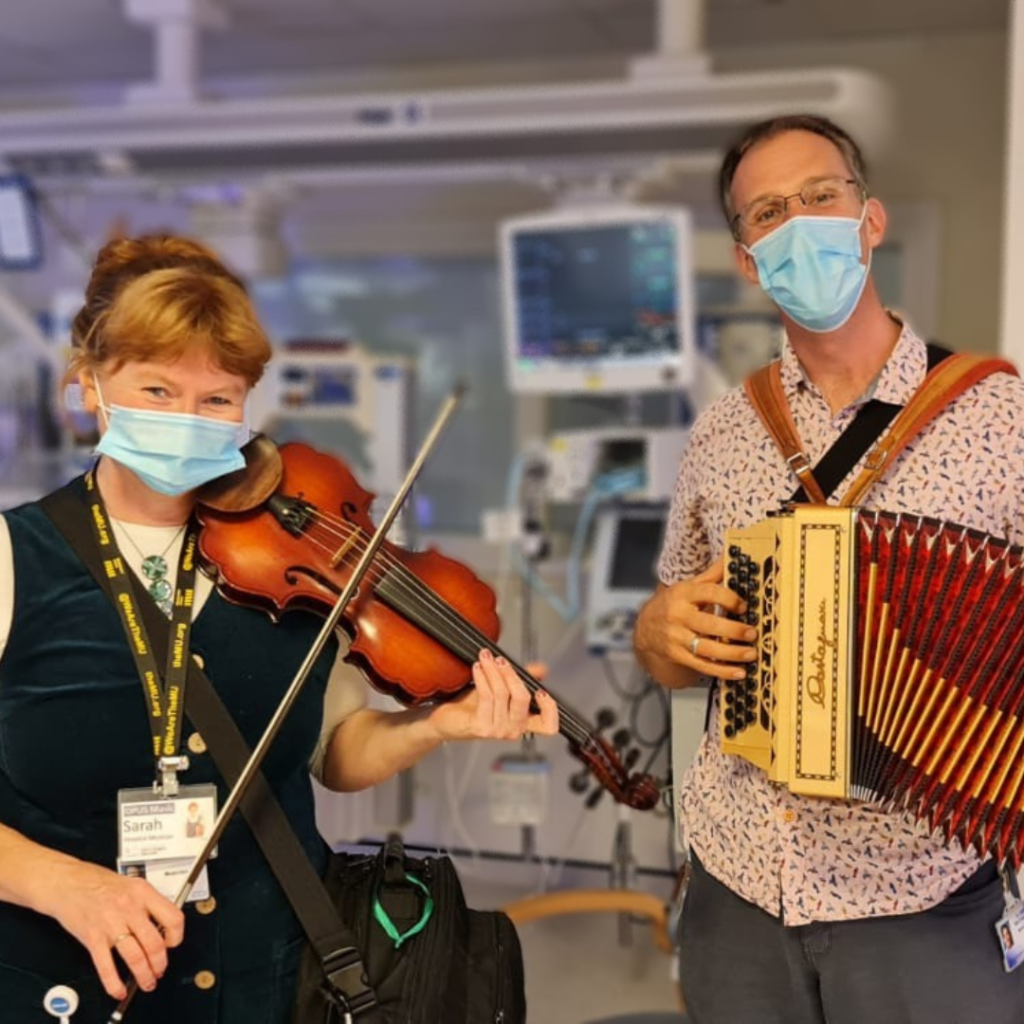
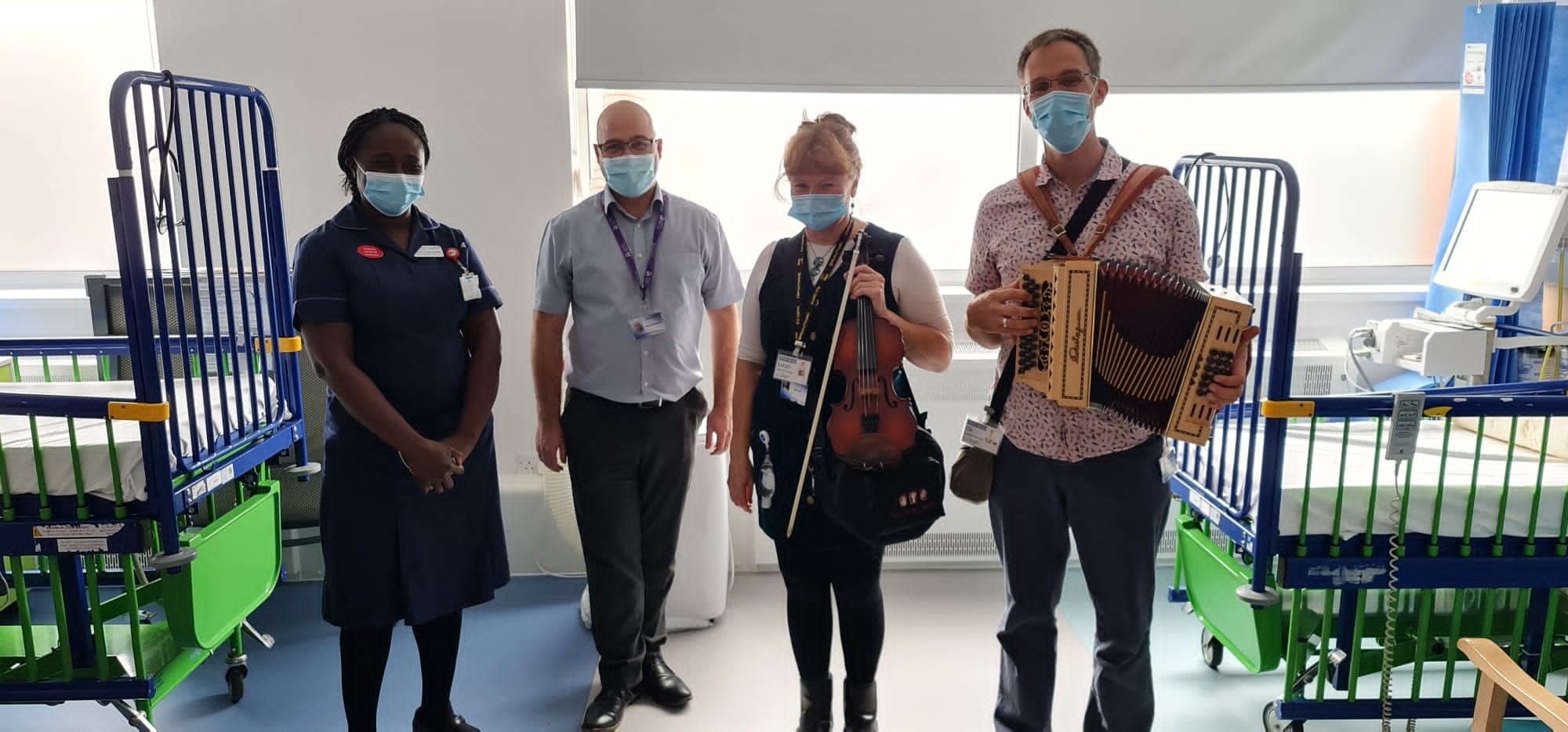
Working on a ward at Nottingham Children’s Hospital, we asked a nurse if it was appropriate to play for the very young baby she was caring for. She said ‘yes of course’. We could see that she was feeding the baby through a feeding tube.
As we played, the nurse interacted with the baby, soothing him through touch and gentle tapping. The ward sister came along and asked the nurse if the baby had calmed down. The nurse said he had since we had arrived. The ward sister then said ‘you have to stay right there until he’s finished!’
Richard asked the nurse if he’d been very distressed and she explained that he’d been struggling feeding with the tube, then getting angry and being sick, so losing the feed. This had caused him to be hungry and the cycle had then repeated.
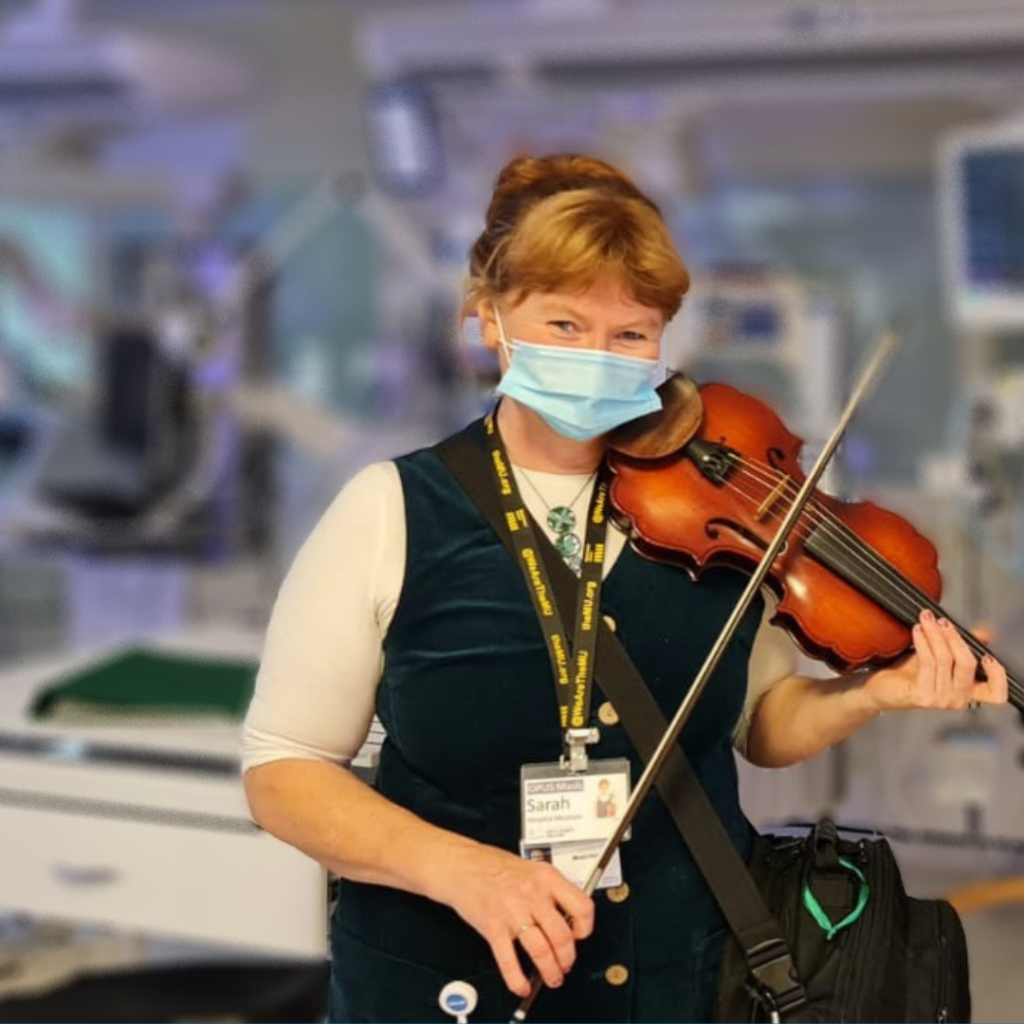
We continued playing and the baby was still slightly upset. Sarah suggested that Richard played the Bodhrán (drum) for the next piece to see if a quiet repetitive rhythm would be soothing. We played ‘Evelyne’s’, moving into ‘Sailor went to sea’. We played an extended version, getting quieter and quieter as the nurse finished the feed and cleaned the feeding tube. She continued to sooth the baby as we played until he fell completely asleep. She smiled and said ‘he’s gone off’ at which point we finished the piece.
As we left the ward he was still asleep and had kept the feed down. The effect of calm induced by the interplay between the nurse and musicians was observed to continue in the baby until his next feed approximately two hours after the musicians had left the space.






































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}